

The Colours we Cannot See
A (colourblind-friendly) deep dive into the science behind colour blindness

My husband and I very rarely disagree, and even when we do, we just agree to disagree. Life is simply too short. There is only one thing we argue about: I have a backpack that is objectively green. I know this because I can see it. However, he claims it is grey. He is positive and would bet the house on it.
Have you ever disagreed so vehemently about the colour of something?

Who is right? Neither.
The backpack has no colour at all. This is true for literally everything around us. The world has no colour; colour is in the brain of the beholder, if you will.
That said, if that backpack were to have a colour, it would so definitely be green.
We all see colours a little differently. For example, what I call white is not the same shade you call white. But there are some people who see colours more differently than others.
Colour blindness is very common. People who are colourblind do not see only in black and white, as the name suggests, but they see different colours than most people. That said, achromatopsia (a deficiency that makes people see only in shades of grey) does exist, but it is extremely rare.
Here are some facts:
Colour deficiency is estimated to affect 300 million people worldwide.
Roughly 8% of all men and 0.5% of all women are colourblind, with some distribution patterns across geographies and ethnic backgrounds.
There are different types of colour blindness, with 95% of all colour deficiency being related to red-green deficiency.
A little history
John Dalton was the first person to scientifically document colour blindness in 1798, based on observations of his own experience, as he was red-green colourblind himself. When he looked at the light split by a prism, he could not see the 7 colours that Newton had described.
“To me it is quite otherwise: —I see only two or at most three distinctions. These I should call yellow and blue; or yellow, blue and purple. My yellow comprehends the red, orange, yellow and green of others; and my blue and purple coincide with theirs” (Dalton, 1798, p. 31)
Dalton thought his vitreous humour (the gel inside his eyes) was tinted blue and filtering out the reds. He asked a physician and friend, Dr. Joseph Ransome to do a postmortem examination of his eyes. In 1844, the day after Dalton died, his friend complied and refuted his theory (Musselman, 2000).
It was Thomas Young in 1802, who first suggested the real cause lay in the retina. Before we knew about photoreceptors, he theorised that 3 light-sensitive particles would be sufficient for us to see all the colours, and that colour deficiencies came from missing or altered ones.
Most of us are trichromats
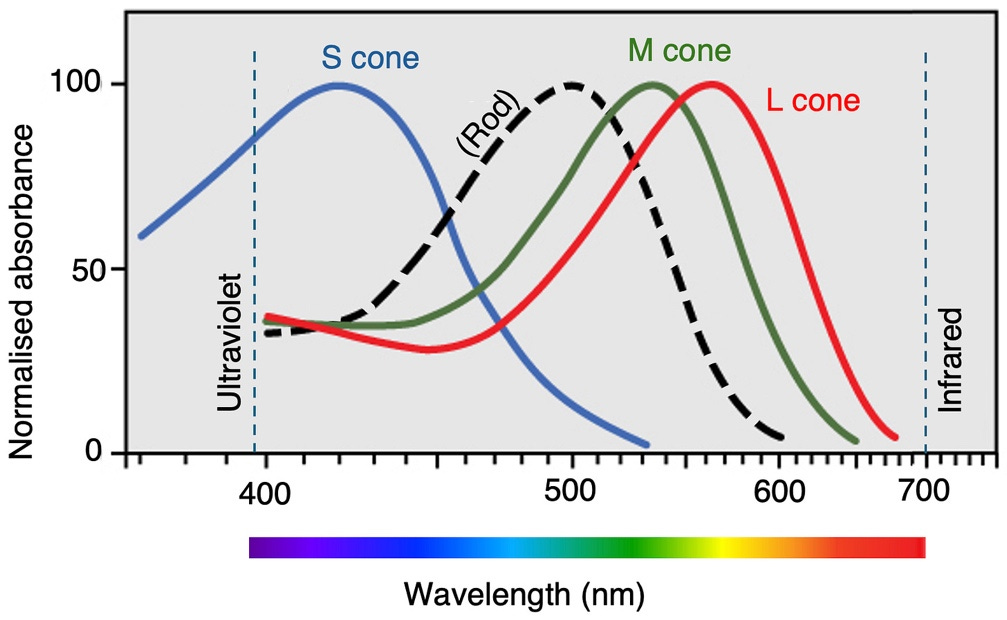
Our eyes have two types of photoreceptors: rods, used for night vision, and cones for colour and detail. Read this excellent deep dive on cones and rods. Cones contain light-sensitive proteins called opsins, each tuned to a specific range of wavelengths. Humans are rare amongst mammals in that they have three types of cones, with peak sensitivities at roughly long (~560 nm), medium (~530 nm) and short (~420 nm) wavelengths. Most mammals, like cats and dogs, are dichromats (two cones). (If you are curious about how your pet sees colour, that is coming in the future.)
These cones are often called red, green and blue, but this is misleading because cones cannot see colours, nor convey colour information. For example, if you miss the “blue” cone, you can still see turquoise but not yellow. Confused? Good.

This is the part explainers leave out
This is why you come to me. Why does losing the function of a single cone (any of them) shift your entire colour perception instead of just knocking down that colour?
Cones convert light into electrical impulses. Cones can only indicate when light is hitting them. You could say they are colourblind in the literal sense. The colours we see are the result of a computation, a comparison of the inputs from the different cones.
The brain creates colour by comparing cone signals. The electrical information generated by the cones is rearranged into three new separate pathways. As you can see in the image above, there is a broad overlap in the sensitivity of the three cones. Any wavelength will stimulate most cones at the same time, but each to a different degree. To determine a colour, neurons need to compare how each of the cones responds to that light.
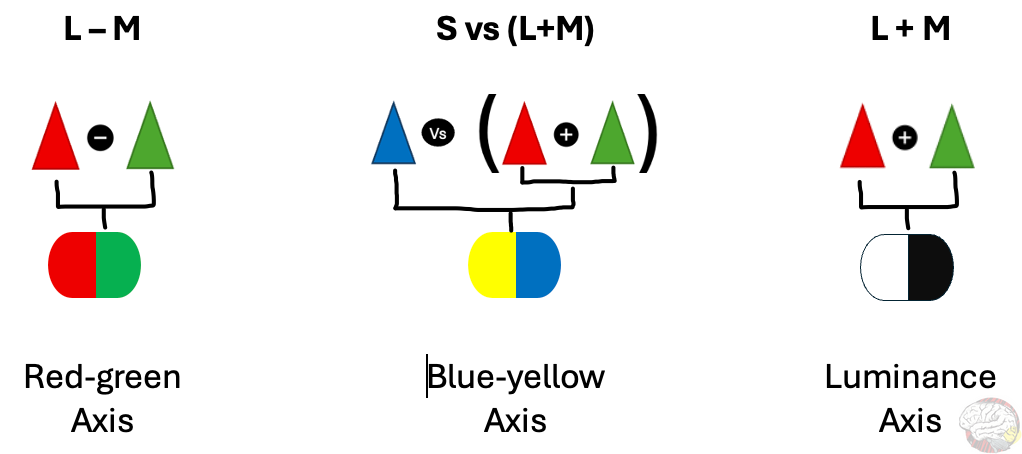
Neurons literally add and subtract cone inputs to build “opponent channels.” Information from each channel is grouped into 3 new pathways. The cool thing is that the same cone inputs are compared in different ways to obtain different kinds of information.
The red-green channel subtracts the M-cone input to the L-cone input → L – M.
The blue-yellow channel compares S-cone input against the combined input of the other two → S – (L + M).
Luminance is obtained by adding the input from L and M → L + M
Graphically:
These three pathways remain largely separate, all the way from the retina, through the lateral geniculate nucleus (the brain’s sensory relay station), and only begin to converge once they reach the visual cortex (V1) at the back of the brain.
Normal (trichromatic) colour vision requires all three cone types.
If any of the cones are missing or altered, an entire axis is shifted.
This is also why we cannot see a reddish-green or a blueish-yellow. Those colours cancel each other out along the opponent axes.
From this wiring, it follows that there can be different types of colour vision depending on how many cones are affected, and specifically, which ones.
How can genes go wrong [or coding errors]
We rely on cones and their opsins for colour vision. The instructions for both the cones and their light-sensitive opsin sit in our genes. Mutations, deletions, or rearrangements in these genes during cell division can disrupt colour perception in different ways:
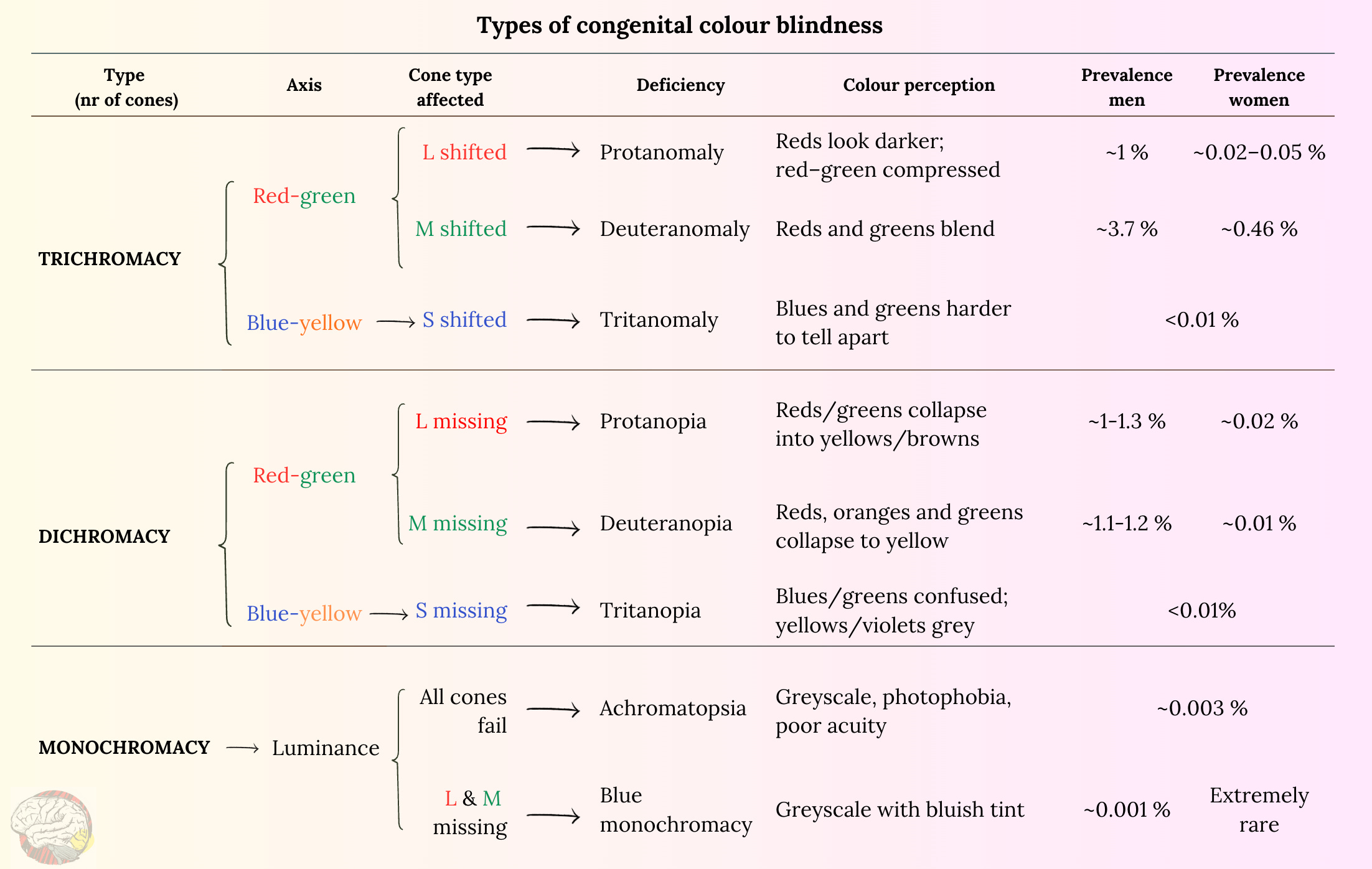
A cone altered → The cone is present and functioning, but the sensitivity of the opsin is shifted to a slightly different peak wavelength. Vision still relies on three cones, but some colours appear less distinct and duller. This results in anomalous trichromacy, and depending on the cone affected, it is called protanomaly (L), deuteranomaly (M), or tritanomaly (S)*.
A cone missing or silenced → Alterations in the gene for a cone or an opsin can silence or delete an entire cone type. This reduces vision to two cones, which is known as dichromacy. The deficiencies are: protanopia, deuteranopia and tritanopia.
All cones knocked out →In very rare cases, mutations in genes that code for the proteins involved in the phototransduction cascade can silence cone function entirely. This is the process that turns light into electrical signals and will affect all the cones, leaving vision to rely only on rods. This is called achromatopsia. This comes accompanied by blurry vision, light sensitivity (if you have read my cones and rods article, you surely know why), and sometimes nystagmus (involuntary eye movement).
* Names in vision science are not very creative - they often refer to the order of discovery (think V1, V2, V3…). In this case, inspiration came from Greek: protos = first; deuter = second; tritos = third. (Meanwhile, scientists who get to name proteins get all the fun: Sonic hedgehog, Ken and Barbie, and my favourite: fuzzy; are all actual protein names. But I digress…)
These genetic coding errors give rise to the congenital (inherited) types of colour vision in humans, from the common red–green deficiencies to the very rare complete loss of cone function.
Not the Same Rainbow
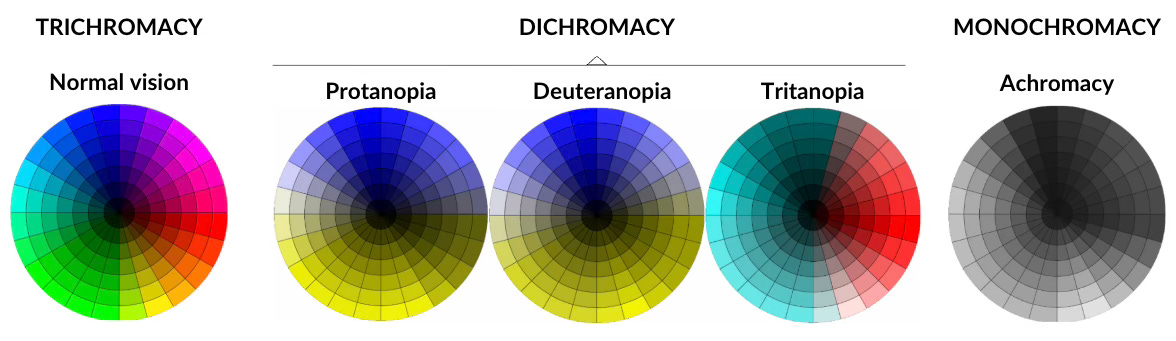
Here are some examples of how colour blind people see.
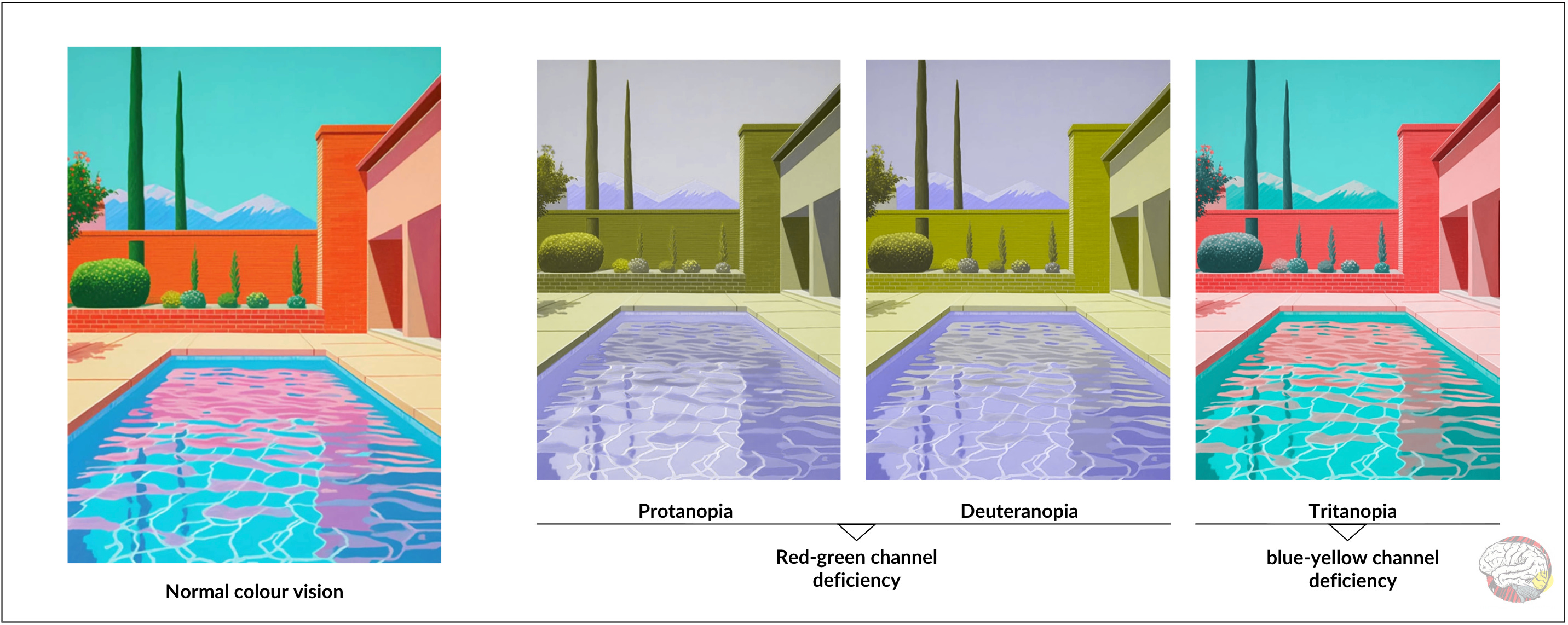
These images are only for reference. Colour blindness is different for each person. It ranges from a mild difficulty in distinguishing colours to an inability to see certain colours. Some people are not even aware of their colour blindness.
Notice above how the protanopia and deuteranopia images look rather similar. This is because the input from red and green cones combines into the same axis. In fact, John Dalton was thought to be a protanope, based on his description of his own colour perception, but in 1995, an analysis of tissue from his eyes confirmed him to be a deuteranope (Hunt et al.). Yes, they still have his eyes. You can visit them at the Science and Industry Museum in Manchester (item Y1997.6.38).
Do you see colours differently from people around you? Which colours do you struggle with most?
Why is red-green colour deficiency more common than blue-yellow?
Red-green problems
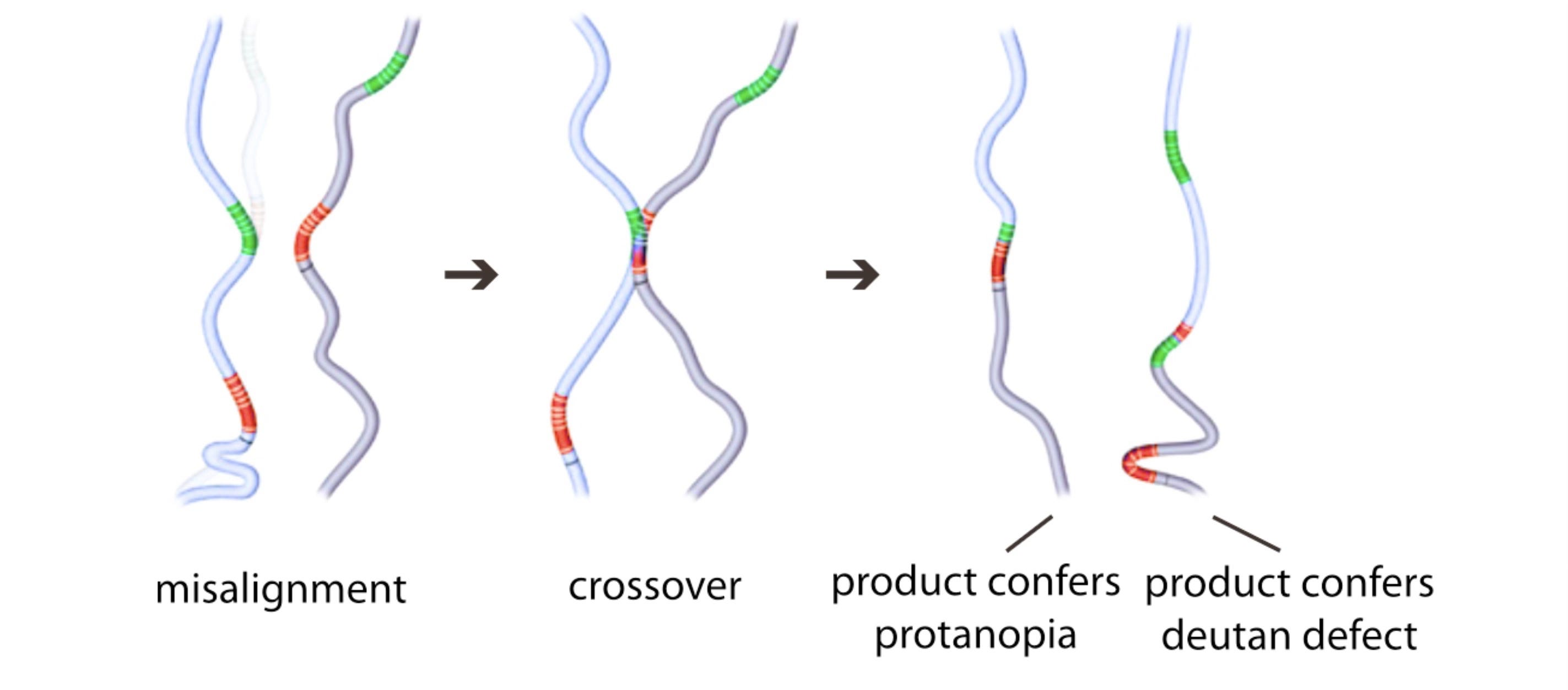
The L and M (red and green) cones are very similar; their sensitivity curves almost overlap, as shown in the first image. The genes that code for them, OPN1LW and OPN1MW respectively, sit side by side in the chromosome and share nearly 98% of their nucleotide material. This closeness and similarity makes them especially prone to mistakes during cell division: the genetic material can be confused, leading to errors such as unequal recombination, mutations and deletions.
Blue-yellow problems
In contrast, the gene that codes for the S cone (blue) sits on an entirely different chromosome, completely separate from the L and M genes on the X. It also shares only about 40% of its sequence with them. This distance and distinctiveness make it much more stable and less prone to the recombination errors that plague the red–green pair.
Why is colour deficiency most common in men?
We humans have 23 pairs of chromosomes, 22 shared by everyone and 1 that determines the sex: males carry an XY pair, while females carry XX. The genes that code for the L and M cones sit on the X chromosome. This means women have a spare one, so as long as one copy works normally, they will experience normal trichromatic vision. They will still carry the defective gene and pass it on.
Red-green: One mutated X is enough to cause
colour blindness in men, but women would need two.
Can we say then that, if a man and a woman disagree about the colour of, say, a backpack, the woman is statistically more likely to be right?
I withdraw the question, Your Honour.
Can we have more than 3 cones?
Yes. But only if you are a woman.
Tetrachromacy means that a visual system relies on 4 cone types. In humans, this possibility exists only in women, because the L and M opsin genes sit on the X chromosome, and women have two of them.
Women who are carriers of anomalous trichromacy inherit one normal opsin gene and one shifted version. As a result, they may express both, giving them S, M, a “normal” L, and a shifted L or M cone — four in total.
So does having four cones actually mean you see a richer rainbow? When 24 women with this genetic setup were tested behaviourally (using colour tests to identify what they saw), only one showed clear evidence of using all four cones in colour perception (Jordan et al., 2010).
How can we explain that? Most likely because our visual system evolved to support three cones, and adding a fourth one does not mean the brain will necessarily exploit it. What we perceive is limited by our brain infrastructure. Have I said that before? Probably. But it is a hill I will happily die on: perception is built in the brain.
The genetics at a glance
Different colour vision deficiencies follow different inheritance rules:
Red–green → X-linked recessive. A single mutated X causes a deficiency in men, but women need both Xs mutated.
Blue–yellow → Autosomal dominant. Caused by mutations on chromosome 7, not a sex chromosome, and therefore affects both men and women equally.
Achromatopsia → Autosomal recessive. Both parents must pass on a defective copy. It involves multiple gene variants (e.g., CNGB3 or CNGA3) and affects men and women equally, although it is very rare.
Can colour blindness be acquired?
So far, we have talked about colour vision deficiencies that are inherited, which are by far the most common, but colour blindness can also be acquired later in life.
Why it happens
Acquired colour vision deficiency becomes more common with age, because many diseases that affect vision are age-related. Here are some examples (the list is much, much longer):
Retinal disease: macular degeneration, diabetic retinopathy, retinal detachment, retinitis pigmentosa.
Optic nerve problems: glaucoma, optic neuritis.
Neurological disease: Parkinson’s disease, Alzheimer’s disease , multiple sclerosis.
Cortical damage: very rare; injury to area V4 can erase colour from our vision.
Medications, toxins: hydroxychloroquine, ethambutol, carbon monoxide, lead.
Lifestyle factors: heavy alcohol use in adolescence/early adulthood may subtly impair colour vision (Brasil et al., 2015).
Inherited vs acquired – the key differences
They affect mostly different axes.
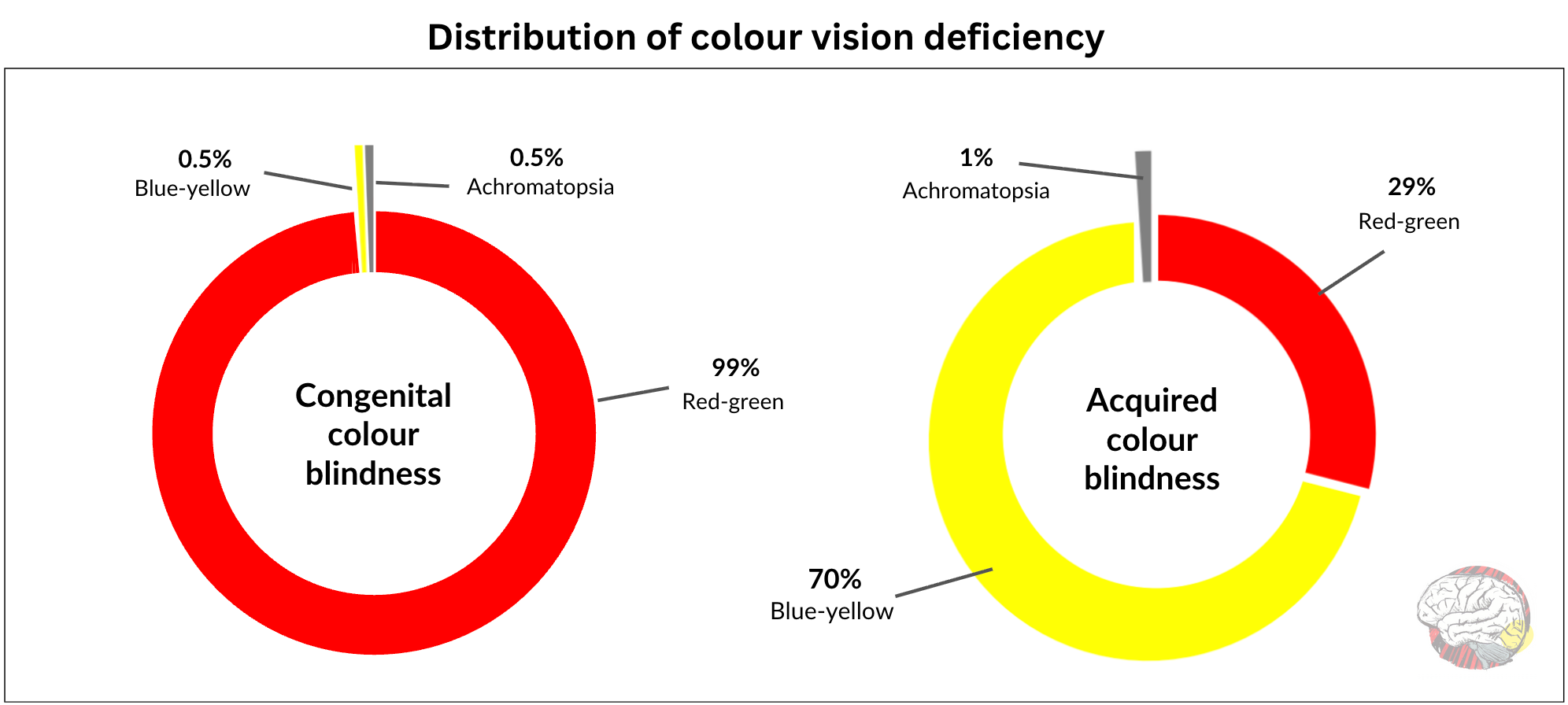
About 95% of inherited cases affect the red–green axis, while acquired deficiencies more often disrupt the blue–yellow axis. In a study of 865 people aged 58–102, Schenk and colleagues (2014) found that perceptual losses along the blue–yellow axis were about three times as common as red–green losses.
Congenital is more stable
Congenital colour deficiency tends to affect all cones of the same type in both eyes, it is present across the entire visual field, and remains stable from birth throughout life. On the contrary, acquired colour vision deficiency is a little messier. It can affect only a portion of the visual field or a single eye, or it can affect both eyes differently. It can also progress or reverse over time.
Awareness matters
Knowing how prevalent colour vision deficiency is matters not only for increasing awareness and implementing accessible design, but also for shaping policies such as early testing, which can be reliably done from the age of 4.
Without early testing, symptoms in children can go unnoticed or be misinterpreted as inattention or poor performance. Think science, biology, art or any topic that involves colour-coded graphics and maps. In some cases, children have erroneously been placed in lower academic tracks. This can cause frustration and self-esteem issues.
Accessible design goes beyond individual accommodations; it makes information more inclusive in all industries. In science, for example, a lot of information is locked inside colour-coded figures.
Daily life, work and workarounds
Colour deficiency is not disabling, but it can be inconvenient. Colourblind people may struggle to identify when fruit is ripe or if meat is cooked through. They learn to rely on other cues or remember the order of the colours.
Most challenges come from living in a world built for trichromats, when a lot of the communication is encoded in colour, from traffic lights to charts and signage.
Colour blindness can also limit career options. Regulations vary by country and profession, but generally, jobs in aviation, transport, engineering, and the military have strict standards, as colour is regularly used for signalling. Some roles in technical or medical fields may also be restrictive.
That said, many people go through life without realising they are colourblind. And those who do know, are often well adapted and may not feel the need to see more colours.
Recommendations
If you work with visuals or teaching materials and want to do your part, here are a few easy changes that make a big difference for people with colour vision deficiency:
Check your visuals. Run your images through a colour blindness simulator if you can. If not, just switch to greyscale and look for contrast. You would be surprised how much information lives in luminance alone.
Do not pack all your information into colour alone. Use textures, labels or symbols to make figures and charts more accessible.
Check your circle. Find out if anyone you regularly work with has any colour needs. You can use desktop simulators to help you design.
Encourage your team to keep accessibility in mind when creating content.
Or make it easier on yourself → 👇 just share this article with them.
Conclusion
All that is happening is that we are seeing the same world differently.
People with colour blindness are not seeing the wrong colours, they are just picking up a different wavelength. The colours we all see are equally real, even if they are different.
There are many (many!) different reasons for colour vision deficiency. The fact that so many different genes, proteins, and pathways can affect colour perception speaks of the many moving parts and the unique balance that is our visual system.
From a biological perspective, there is no survival threat for colour blindness. The inconvenience comes from living in a society designed around a trichromatic standard.
Colour vision is just another reminder that reality is different for everyone.
If you had a colour deficiency, would you want to know? Would you feel robbed to find out X% of people see colours you cannot see? Are you colourblind? If so, how does it affect you? Let me know in the comments.
An entirely unrelated question
Before you go, can you help me with a survey? Only one question:
Look at the object below and tell me, what colour do you see?

If you enjoyed this, share it with someone who sees the world a little differently.
It takes a lot of work and time to write these articles. If you find value in what you just read and want to support my work, you can buy me a coffee.
In any case, if you got this far, please like and restack, and feel free to drop any questions in the comments.
References:
Brasil, A., Castro, A. J. O., Martins, I. C. V., Lacerda, E. M. C., Souza, G. S., Herculano, A. M., ... & Silveira, L. C. L. (2015). Colour vision impairment in young alcohol consumers. PLoS One, 10(10), e0140169.
Dalton, J. (1798). Extraordinary facts relating to the vision of colours: With observations. Memoirs of the Literary and Philosophical Society of Manchester, 5(1), 28–45. https://digital.sciencehistory.org/works/fb4949523
Hunt, D. M., Dulai, K. S., Bowmaker, J. K., & Mollon, J. D. (1995). The chemistry of John Dalton’s color blindness. Science, 267(5200), 984-988.
Jordan, G., Deeb, S. S., Bosten, J. M., & Mollon, J. D. (2010). The dimensionality of color vision in carriers of anomalous trichromacy. Journal of vision, 10(8), 12-12.
Neitz, J., & Neitz, M. (2011). The genetics of normal and defective color vision. Vision research, 51(7), 633-651.
Musselman, E. G. (2000). Local colour: John Dalton and the politics of colour blindness. History of science, 38(4), 401-424.
Schneck, M. E., Haegerstrom-Portnoy, G., Lott, L. A., & Brabyn, J. A. (2014). Comparison of panel D-15 tests in a large older population. Optometry and Vision Science, 91(3), 284-290.
Hi Vanesa,
Loved this! My partner and I also have ongoing ‘colour debates’ (we have a sofa that’s apparently both beige and grey 🤷). Reading this made me appreciate that maybe we’re both right — just seeing through slightly different neural filters.